
Beyond Subcutaneous Models: Rethinking Implantation Site in Preclinical Oncology
In our first post of this series, we examined how tumor immunophenotype and combination treatment strategy influence checkpoint inhibitor efficacy in syngeneic models. We closed with a question: what happens when you take the same cell line and implant it somewhere other than the flank?
The answer, as our data show, can be profound. The anatomical site of tumor implantation is one of the most underappreciated variables in syngeneic model design. The same tumor cell line can exhibit markedly different immune phenotypes, levels of immune infiltration, and sensitivity to PD-1 blockade depending on its anatomical location. For researchers seeking to model specific clinical contexts (e.g. primary tumor biology, metastatic dissemination, or central nervous system (CNS) disease), this is not a minor technical detail. It is a critical determinant of whether a model generates data that is scientifically meaningful.
Below, we present findings across three syngeneic models (GL261 glioblastoma, ID8 ovarian cancer, and CT26 colon cancer), each illustrating a distinct dimension of site-dependent tumor biology.
The CNS as an Immunologically Restricted Environment
In the GL261 glioblastoma model, we compared immune checkpoint inhibitor (ICI) efficacy in tumors implanted subcutaneously versus intracerebroventricularly (ICV).
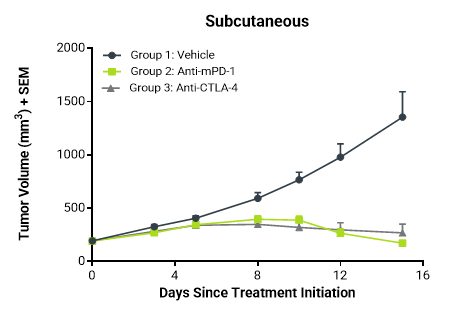
Subcutaneous GL261 tumors showed strong regression following PD-1 blockade. ICV tumors, however, exhibited only moderate responses, a pattern consistent with both the immunologically restricted CNS environment and the well-documented clinical resistance of glioblastoma to ICIs (Figure 1).
Fig. 1. ICI response across GL261 implantation sites. Comparison of ICI efficacy in GL261 tumors implanted intracerebroventricularly (A, B) versus subcutaneously (C). Subcutaneous tumors showed strong regression following PD-1 blockade, while ICV tumors exhibited only moderate responses, aligning more closely with clinical glioblastoma outcomes.
Fig. 1A:
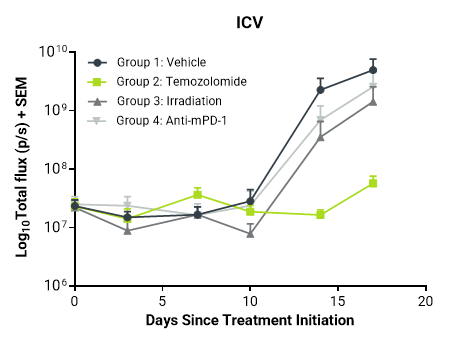
Fig. 1B:
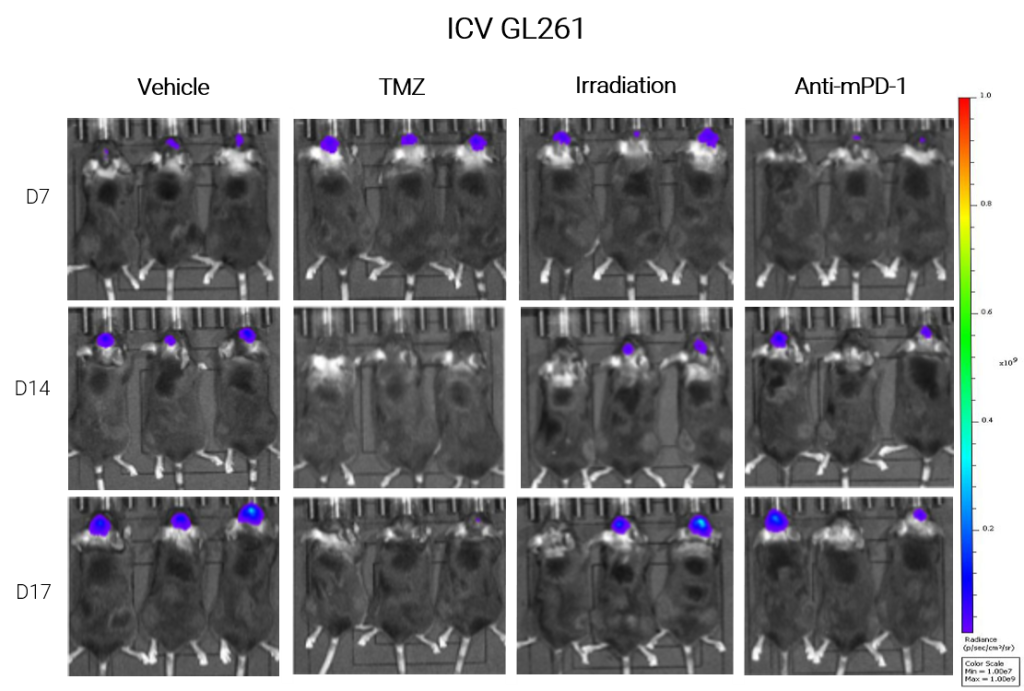
Fig. 1C:
This site-dependent difference is biologically unsurprising. The CNS is an immunologically restricted environment characterised by limited peripheral immune surveillance, a specialised blood-brain barrier, and distinct resident immune cell populations including microglia. Together, these features create a microenvironment that is fundamentally less permissive to T cell-mediated anti-tumor activity than the subcutaneous tissue1.
These findings underscore an important principle: subcutaneous implantation of a CNS tumor line is not an adequate proxy for intracranial disease. For glioblastoma and other brain tumors, achieving translational relevance requires models that recapitulate the immunological constraints of the CNS environment. Our team has therefore developed an intracranial injection model to evaluate ICI response in an anatomically intact brain environment.
Peritoneal Heterogeneity
The ID8 ovarian cancer model provided a different but equally informative example. Both subcutaneous and orthotopic implantation generated immunologically cold tumor phenotypes with minimal ICI response, consistent with the broadly immunosuppressive microenvironment associated with ovarian cancer. Intraperitoneal implantation, however, revealed a more complex picture: heterogeneous responses, with a subset of mice exhibiting partial sensitivity to PD-1 blockade (Figure 2).
Fig. 2. ICI response across ID8 implantation sites. Comparison of ICI efficacy in ID8 ovarian tumor models implanted orthotopically (A,B), intraperitoneally (C,D), and subcutaneously (E). Subcutaneous and orthotopic tumors showed minimal response, consistent with a “cold” phenotype. In contrast, the intraperitoneal model exhibited heterogeneous responses, with a subset of mice demonstrating partial sensitivity to PD-1 blockade.
Fig. 2A:
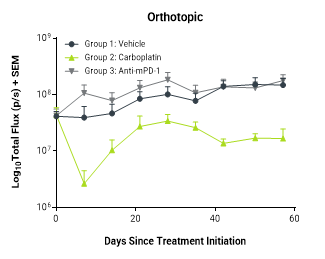
Fig. 2B:
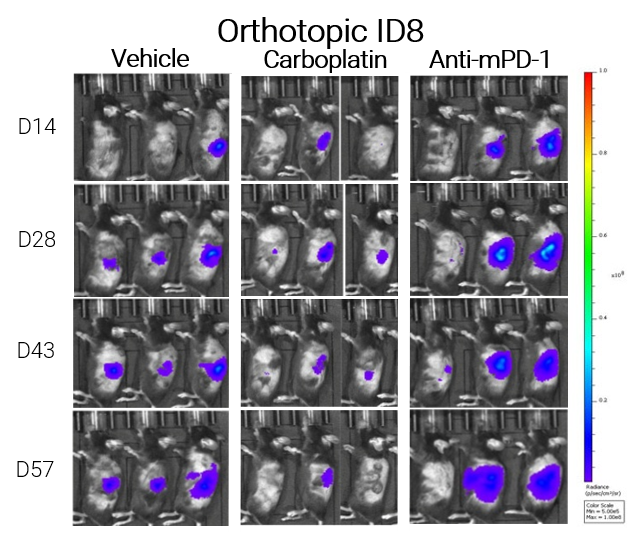
Fig. 2C:
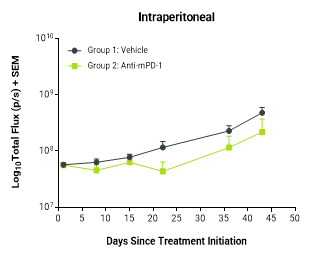
Fig. 2D:
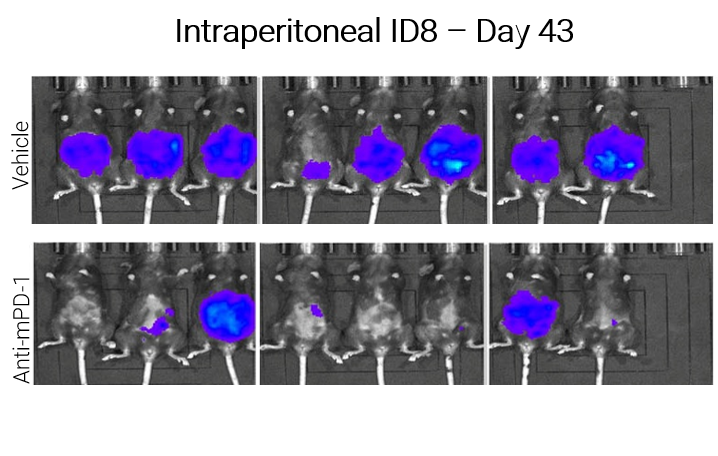
Fig. 2E:
This heterogeneity is unlikely to represent experimental noise; it mirrors the variable clinical responses to ICIs observed in ovarian cancer patients and positions the intraperitoneal model as a compelling platform for biomarker discovery. Understanding why some tumors within an otherwise immunologically cold model respond while others do not, may provide mechanistic insight into the determinants of patient sensitivity to checkpoint blockade. This is precisely the type of question that requires a model capable of capturing biological variability, rather than one that generates uniformly negative results.
Site-Dependent Immunophenotype Switching
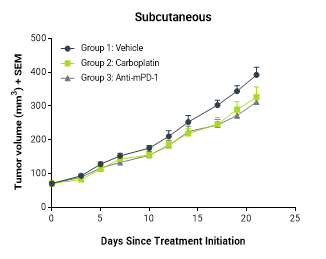
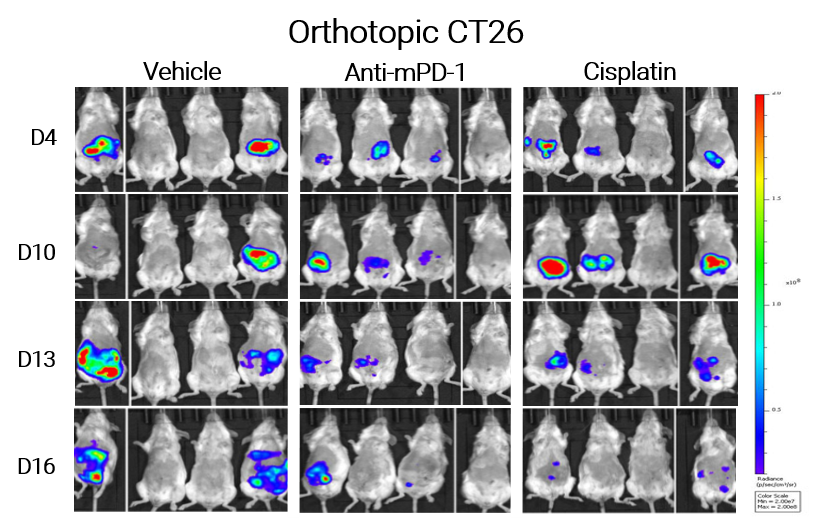
The CT26 model offered one of the clearest illustrations of implantation site effects. When established subcutaneously, intracarotidally (ICA) (as a brain metastasis model), or intrasplenically (as a liver metastasis model), CT26 tumors retained their characteristically hot immunophenotype and responded robustly to PD-1 blockade. Orthotopic colon implantation, however, produced a fundamentally different result: a cold tumor phenotype with markedly reduced responsiveness to immune checkpoint inhibition (Figure 3).
Fig. 3. ICI response across CT26 implantation sites. CT26.WT tumors show strong ICI responses when implanted subcutaneously (A), intracarotidally (B, D; brain metastasis model), or intrasplenically (C; liver metastasis model). However, orthotopic colon implantation results in a cold tumor phenotype with reduced responsiveness (E, F). Ongoing analysis of tumor microenvironments aims to elucidate the mechanisms underlying these site-dependent differences.
Fig. 3A:
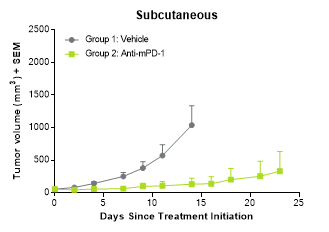
Fig. 3B:
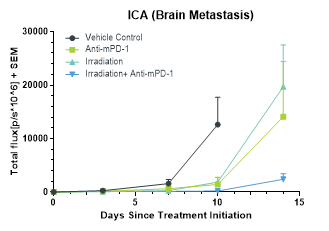
Fig. 3C:
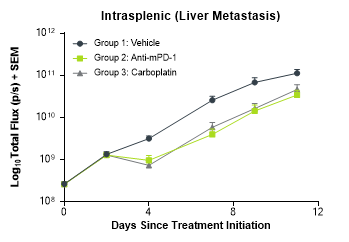
Fig. 3D:
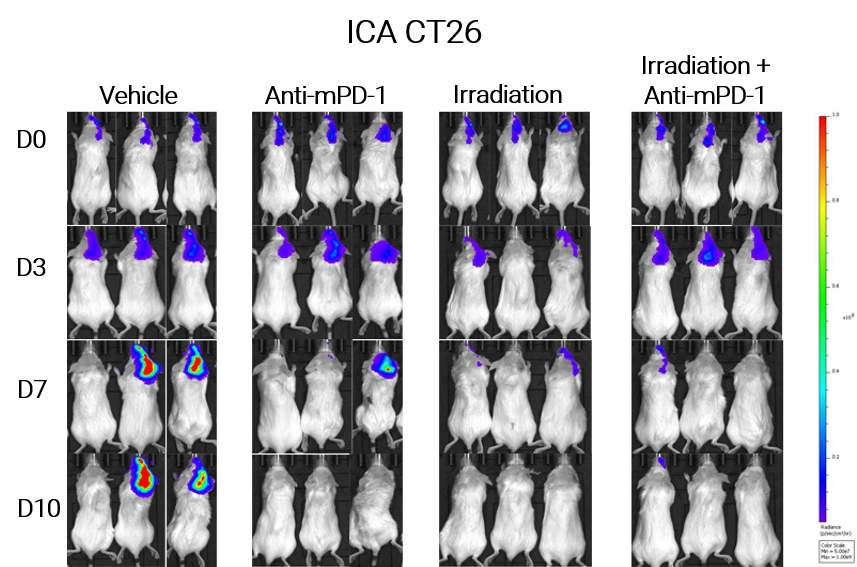
Fig. 3E:
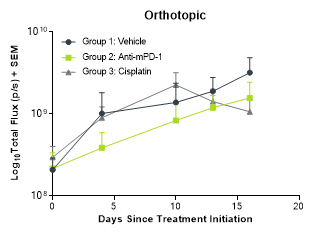
Fig. 3F:
The same cell line. Profoundly different biology. This finding directly challenges the common assumption that subcutaneous CT26 models adequately represent primary colorectal disease. The colonic microenvironment appears to impose immunosuppressive pressures that substantially reshape the tumor immune landscape, suppressing the T cell infiltration and pro-inflammatory immune signalling that define CT26 as a hot model in other anatomical contexts.
These findings raise an important question for the field: if a hot tumor cell line can switch to a cold phenotype simply by being placed in its anatomically correct location, to what extent do subcutaneous models – still the industry default – truly reflect clinic disease biology?
What This Means for Model Selection
Taken together, these data make a clear case: implantation site is not merely a logistical decision; it is a scientific one. The anatomical location in which a tumor grows determines the immune microenvironment it encounters, the degree of immune surveillance it experiences, and ultimately its responsiveness to immunotherapy.
For CNS tumors, subcutaneous implantation may substantially overestimate ICI efficacy. For tumors with distinct primary-site biology, such as colorectal cancer, orthotopic implantation may be essential to capture the immunosuppressive context that characterises patient disease. And in models where peritoneal dissemination is clinically relevant, intraperitoneal implantation can reveal biological heterogeneity that subcutaneous models may fail to capture.
At ChemPartner, we offer a comprehensive portfolio of implantation models: subcutaneous, orthotopic, intraperitoneal, intracardiac, intracranial, intracarotid; to support preclinical study designs that align with the biological context of the disease being modelled.
In our final syngeneic blog post we turn to metastatic disease, where orthotopic and systemic syngeneic metastatic cancer models remain a highly active area of preclinical immuno-oncology research, driven by the need to better recapitulate the complex tumour microenvironment, metastatic cascade, and immunotherapy responses observed in patients.
Interested to learn more?

1) Kalluri AL, Shah PP, Lim M. The Tumor Immune Microenvironment in Primary CNS Neoplasms: A Review of Current Knowledge and Therapeutic Approaches. Int J Mol Sci. 2023 Jan 19;24(3):2020. doi: 10.3390/ijms24032020. PMID: 36768342; PMCID: PMC9917056.