
Syngeneic Tumor Models: The Gold Standard for Preclinical Immunotherapy Testing
Cancer immunotherapy has transformed oncology, yet translating early efficacy into consistent clinical success remains challenging. Central to this effort is the need for preclinical models that genuinely reflect how tumors and the immune system interact, and syngeneic tumor models have emerged as the platform of choice. Here, we explore how tumor immunophenotype and treatment combination influence therapeutic outcome in syngeneic models.
What Are Syngeneic Tumor Models?
Syngeneic models are created by implanting murine tumor cell lines into genetically matched host mice of the same inbred strain. Because host and tumor share the same MHC haplotype, the immune system isn’t artificially suppressed and the tumor is not immediately rejected, allowing it to grow in an immunocompetent setting.
This preserves functional host immunity without the need for systemic immunosuppression, making these models valuable for studying anti-tumor immune responses and immunotherapies.
However, the tumor-immune interactions in this setting may not fully recapitulate the complexity of spontaneous human cancers.
Since the first immune checkpoint inhibitors (ICIs) were approved in 2011[1], syngeneic models have been central to evaluating checkpoint blockades in preclinical settings.
These models have evolved considerably since their initial use in single-agent efficacy studies and are now widely applied to evaluate combination therapies and to interrogate the tumor microenvironment (TME).
More recently, efforts have also been made to better capture tissue-specific immune contexts across different anatomical sites, although this remains an area of ongoing development.
Why Syngeneic Models Are Essential for ICI Research?
ICI efficacy is strongly influenced by the tumor immune microenvironment, and syngeneic models remain one of the most widely used in vivo systems for studying immune-tumor interactions in an immunocompetent setting.
However, a major challenge in ICI development is the substantial immunological heterogeneity of human tumors, which contributes to highly variable patient responses.
Tumors are broadly classified along an immunophenotypic spectrum. At one end, “hot” tumors are characterized by high T cell infiltration, elevated tumor mutational burden (TMB), active immune signaling, and expression of immune checkpoint molecules such as PD-L1.
These features reflect an ongoing anti-tumor immune response that has been suppressed rather than absent, making hot tumors more likely to respond to checkpoint blockade.
Clinical data consistently show that patients with hot tumors achieve higher response rates and more durable outcomes with ICI therapy[2].
At the other end of the spectrum, ‘cold’ tumors typically exhibit low immune cell infiltration and are often associated with immunosuppressive features, including regulatory T cell (Treg) accumulation, myeloid-derived suppressor cell (MDSC) recruitment, and cytokines such as TGF-β and IL-10. They are also frequently, though not universally, linked to lower tumor mutational burden.
These features collectively establish a TME that is largely resistant to checkpoint blockades. Converting cold tumors into ICI-responsive ones is one of the central challenges in the field, and identifying strategies to do so requires preclinical systems that faithfully model the immunosuppressive TME 2.
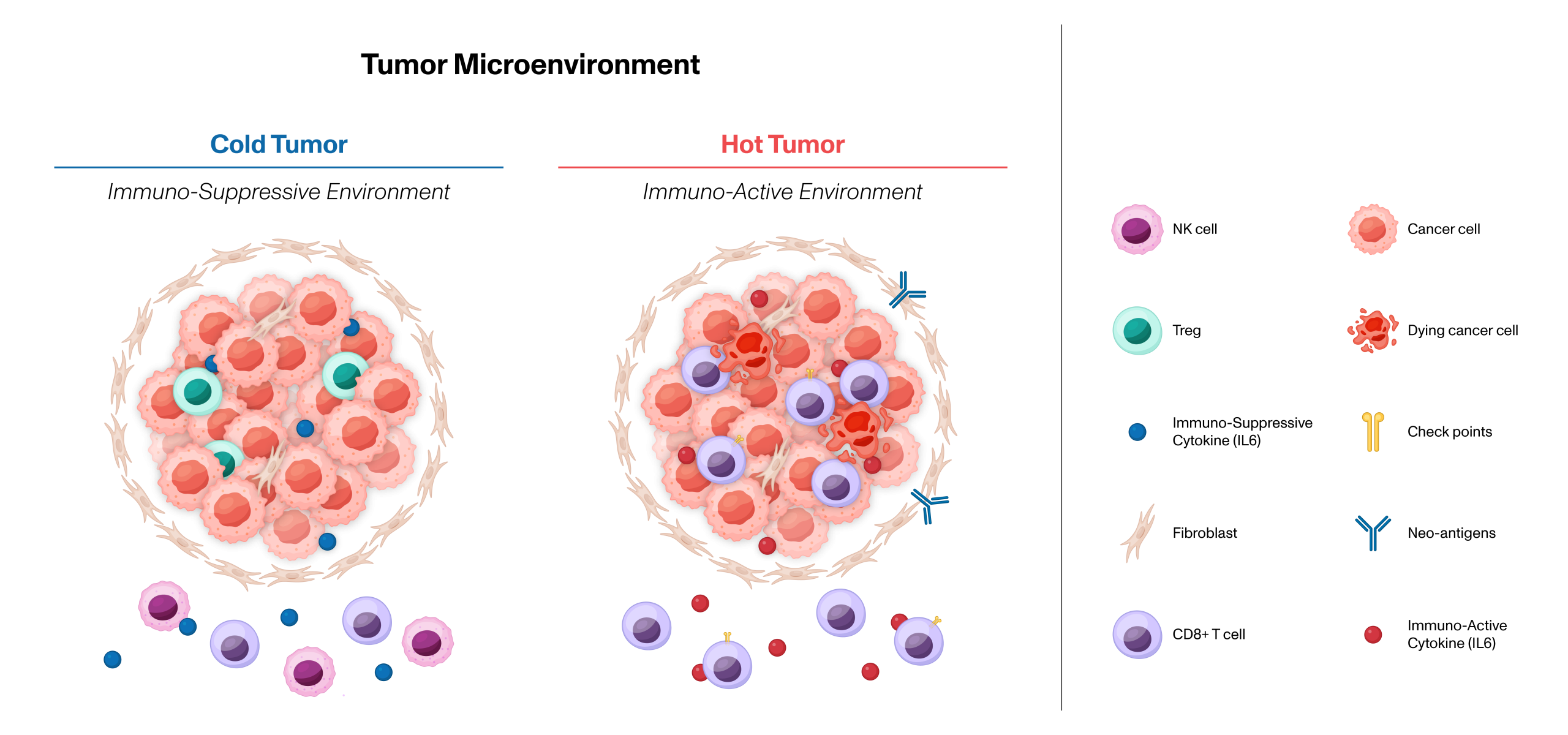
Figure 1 Hot and Cold Tumor Microenvironment.
A well-curated panel of syngeneic models can span both ends of this spectrum, giving researchers a realistic picture of how a therapy is likely to perform across different patient populations. ChemPartner’s syngeneic panel is designed to capture a broad spectrum of tumor–immune interactions, enabling more nuanced immuno-oncology research.
It includes models that represent both highly immunogenic “hot” tumors with strong baseline responses to immune checkpoint inhibitors, as well as more immunosuppressive “cold” tumors that better reflect resistant microenvironments such as those found in the CNS.
The panel also incorporates engineered variants to support evaluation of targeted therapies and combination strategies, alongside models where treatment response varies by biological context, offering valuable insight into mechanisms like immune exclusion.
Testing Combination Therapies
One of the most important applications of syngeneic models is the evaluation of combination therapies, where ICI activity is studied alongside other treatment modalities.
Combining Radiotherapy with Immunotherapy
The combination of radiotherapy and immune checkpoint blockade has attracted considerable interest, supported by evidence that radiation can render immunologically “cold” tumors more responsive to immune-mediated killing.
Syngeneic models are uniquely positioned to investigate this interaction, as the underlying mechanisms depend on an intact and fully functional immune system.
Using the CT26.WT colon cancer model, we investigated whether low-dose radiotherapy could enhance the anti-tumor effect of PD-1 blockade. Combining anti-mPD-1 antibody with 1 Gy or 3 Gy irradiation produced significantly greater tumor growth inhibition than either treatment alone (Figure 2).
The combination also produced a marked survival benefit, with the 3 Gy plus anti-mPD-1 cohort showing the strongest effect, suggesting a dose-dependent contribution of radiation to immune sensitization.
These findings are consistent with radiation-induced immunogenic cell death (ICD), in which calreticulin surface exposure, HMGB1 release, and ATP secretion function as danger signals that enhance tumor antigen presentation and promote T cell priming.
This process can contribute to a more inflamed tumor immune microenvironment, increasing susceptibility to checkpoint blockade.
The data also highlights a broader principle: radiation dose selection in combination studies is not merely a tolerability consideration, but an important determinant of immunological outcome.
The ability to model this dose-response relationship in an immunocompetent host represents a key strength of the syngeneic platform.
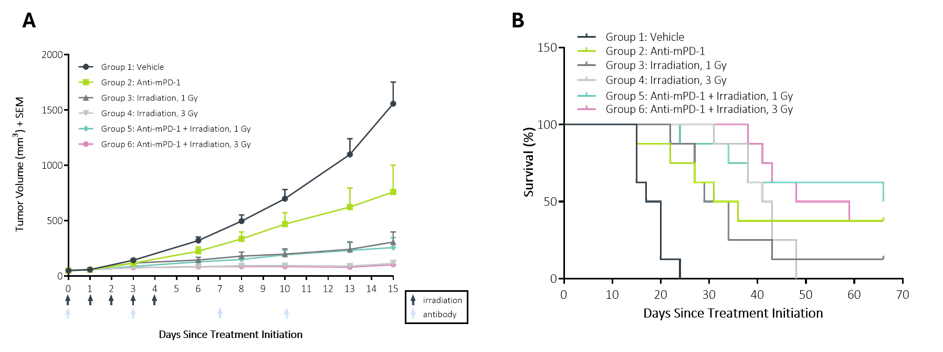
Figure 2 Subcutaneous tumor growth and survival analysis following PD-1 blockade and irradiation. (A) Mean tumor volume curves for vehicle, anti-mPD-1, irradiation (1 Gy or 3 Gy), and combination therapies. Anti-mPD-1 combined with irradiation (1 Gy or 3 Gy) resulted in the greatest tumor growth inhibition compared to monotherapies or control. (B) Mice treated with anti-mPD-1 & irradiation, particularly at 3 Gy, exhibited the greatest survival benefit, indicating a synergistic effect between immunotherapy and radiotherapy.
Antibody-Drug Conjugates: Pairing Targeted Therapy with Immune Activation
ADCs have established themselves as a distinct and increasingly important therapeutic class, combining the target specificity of monoclonal antibodies with the cytotoxic potency of small molecule payloads.
More recently, attention has turned to their interaction with the immune system, with emerging evidence suggesting that ADC-induced tumor cell death can engage immunological pathways that may be relevant to responses to ICIs. Syngeneic models are well positioned to investigate these questions, given their fully immunocompetent host environment.
Using the CT26-hHER2 model, we evaluated trastuzumab deruxtecan (Enhertu), a HER2-directed ADC incorporating a topoisomerase I inhibitor payload, in combination with anti-mPD-1. The combination produced the most significant reduction in tumor volume and the greatest survival benefit relative to monotherapy (Figure 3).
These data support the hypothesis that ADC-mediated cytotoxicity induces ICD, generating immunogenic signals that remodel the TME and create conditions more conducive to checkpoint inhibition.
The finding has broader implications for ADC development. If cytotoxic payload-induced ICD can enhance ICI sensitivity, then the immunological properties of the payload, and not solely its cytotoxic potency, may be a relevant consideration in ADC design and combination strategy.
Syngeneic models provide a tractable system in which to investigate this relationship, enabling the immune consequences of different payload mechanisms to be characterized in vivo prior to clinical evaluation.
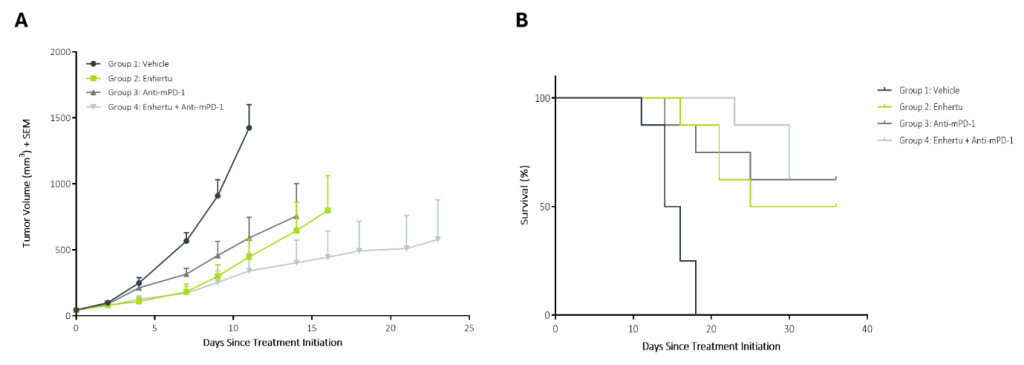
Figure 3 Subcutaneous tumor growth and survival analysis following Enhertu treatment and PD-1 blockade. (A) Mean tumor volume curves for vehicle, Enhertu, anti-mPD-1, or combination therapy. Enhertu combined with anti-mPD-1 resulted in the greatest inhibition of tumor growth, indicating enhanced antitumor efficacy compared to monotherapies. (B) Mice treated with combination therapy exhibited the greatest survival benefit.
Choosing the Right Model for the Right Question
These findings highlight that model selection should be guided by the specific biological question under investigation. In preclinical oncology, the choice of model can strongly influence interpretation: systems that are overly sensitive may overestimate therapeutic efficacy, while those that are poorly responsive may obscure meaningful biological signals.
Both scenarios can complicate translation to the clinic, where tumor heterogeneity and immune context play critical roles.
A carefully designed syngeneic study, in which the model is appropriately matched to the clinical setting and mechanism of action being evaluated, is more likely to generate data that is relevant to clinical decision-making (Table 1).
Table 1 Matching Syngeneic Models to Preclinical Research Questions.
| Research Question | Recommended Approach |
| Baseline ICI sensitivity / proof of concept | Subcutaneous hot model (e.g. CT26.WT) |
| ICI resistance mechanisms | Cold model or orthotopic implantation |
| CNS tumor immunotherapy | Intracranial or ICV implantation |
| Metastatic disease context | Intrasplenic, intraperitoneal or intravenous models |
| Combination with radiotherapy or ADCs | Immunocompetent syngeneic host essential |
What’s Next?
Model design extends far beyond cell line selection alone. In our next post, we explore the anatomical site of tumor implantation as critical – and often underappreciated -determinant of experimental outcome.
Our emerging data show that the same cell line can display strikingly different immune landscapes and responses to ICI depending on where it is established, with important implications for translational relevance and study interpretation.
If you’d like to learn more about how ChemPartner’s syngeneic tumor model platform can support your immunotherapy program, contact our team.
[1] O’Day SJ, Maio M, Chiarion-Sileni V, Gajewski TF, Pehamberger H, Bondarenko IN, Queirolo P, Lundgren L, Mikhailov S, Roman L, Verschraegen C, Humphrey R, Ibrahim R, de Pril V, Hoos A, Wolchok JD. Efficacy and safety of ipilimumab monotherapy in patients with pretreated advanced melanoma: a multicenter single-arm phase II study. Ann Oncol. 2010 Aug;21(8):1712-1717. doi: 10.1093/annonc/mdq013. Epub 2010 Feb 10. PMID: 20147741.
2[2] Wang L, Geng H, Liu Y, Liu L, Chen Y, Wu F, Liu Z, Ling S, Wang Y, Zhou L. Hot and cold tumors: Immunological features and the therapeutic strategies. MedComm (2020). 2023 Aug 26;4(5):e343. doi: 10.1002/mco2.343. PMID: 37638340; PMCID: PMC10458686.