
The Metastatic Challenge: Matching Preclinical Models to Late-Stage Disease
In the first two posts of this 2026 series (syngeneic tumor models blog and beyond subcutaneous models blog), we examined how tumor immunophenotype shapes response to immune checkpoint inhibitors (ICI), and how the anatomical site of implantation can fundamentally alter that response, even for the same cell line.
The CT26 model exemplifies this: a characteristically hot tumor that becomes immunologically cold when placed in its anatomically correct colonic environment. These findings point to a broader challenge in preclinical oncology study design, particularly when modelling metastatic disease.
Metastatic disease accounts for the majority of cancer-related mortality, yet most preclinical efficacy studies continue to rely on primary subcutaneous tumor models. Subcutaneous tumors grow in an anatomical environment that poorly recapitulates the sites where metastatic lesions develop, and the immune landscape of these secondary sites can differ substantially from that of the primary tumor. Designing preclinical studies for metastatic indications therefore requires models capable of capturing this biological complexity.
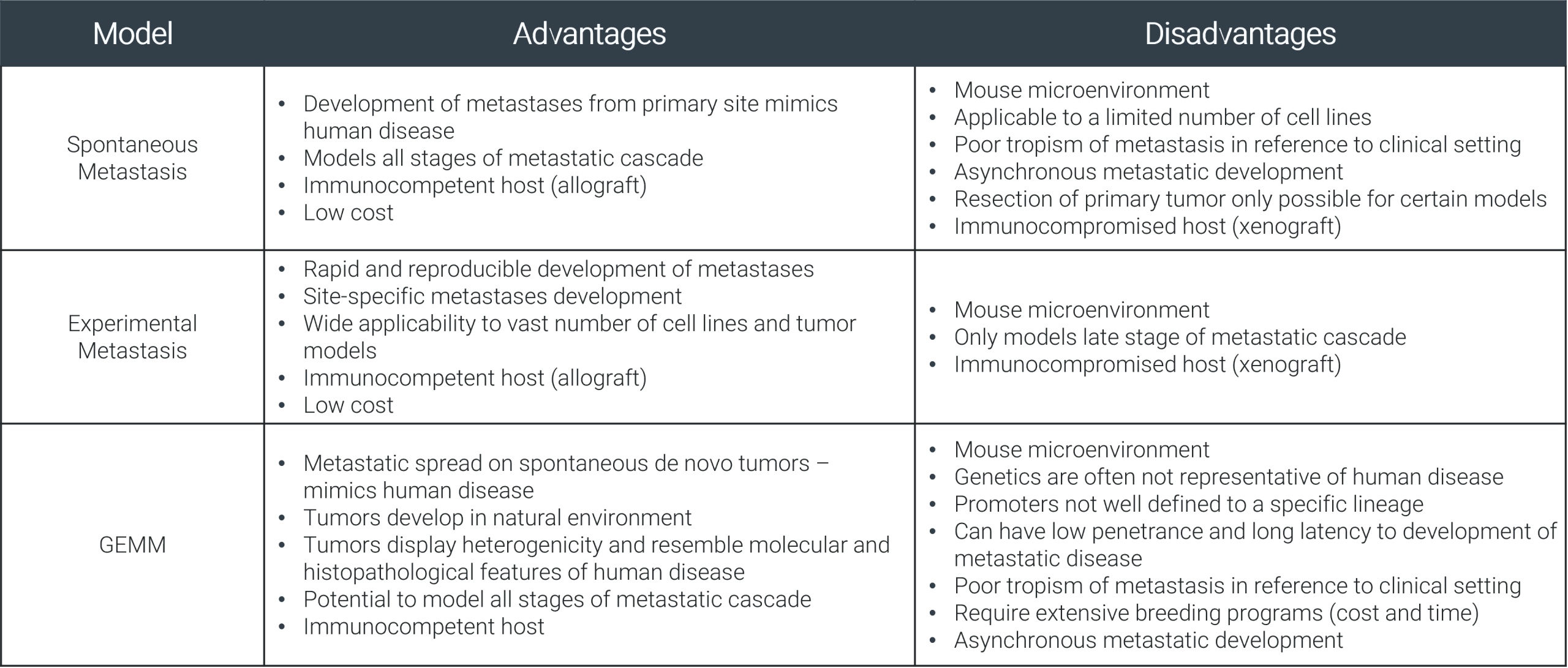
Three broad strategies are commonly used to model metastaic disease (Figure 1):
- Spontaneous metastasis models allow the full process of tumor dissemination from a primary site, more closely mimicking how human disease naturally evolves.
- Experimental metastasis models bypass the early stages of dissemination by delivering tumor cells either directly to the target organ or via systemic injection.
- Genetically engineered mouse models (GEMMs) take a different approach entirely, driving tumor formation through defined oncogenic mutations in an immunocompetent host and providing a biologically accurate representation of tumor initiation and progression.
Each approach involves trade-offs between biological fidelity and experimental practicality, and the choice should be guided by the scientific question.
Figure 1 Mouse Models of Metastasis.
Spontaneous Metastasis: The 4T1 Breast Cancer Model
In spontaneous metastasis models, tumor cells are implanted at the primary anatomical site (orthotopically), allowing metastasis to develop naturally over the course of the study.
This approach preserves the full biological sequence of metastatic progression: local invasion, intravasation, circulation, extravasation, and colonization of a distant organ. For models using immunocompetent hosts, the immune dynamics shaping each stage of that process also remain intact.
The 4T1 syngeneic breast cancer model is among the most widely used platforms for studying spontaneous metastasis. Following orthotopic implantation into the mammary fat pad of immunocompetent BALB/c mice, 4T1 tumors spontaneously disseminate to the lungs, liver, bones, and lymph nodes, recapitulating a clinically relevant pattern of metastatic spread.
A key design decision in 4T1 studies is whether to surgically resect the primary tumor. These two approaches model different clinical scenarios and generate distinct datasets.
Without resection, primary tumor volume and terminal lung weight can be measured in parallel, capturing simultaneous assessment of primary tumor growth and metastatic disease progression.
With resection, the primary tumor is removed at a defined timepoint, and the study subsequently tracks metastatic burden and survival, more closely reflecting the adjuvant and neoadjuvant clinical settings in which many anti-cancer agents are evaluated.
Data from ChemPartner’s 4T1 platform illustrate both study designs. In the non-resection setting, cisplatin significantly reduced both tumor growth and terminal lung weight, indicating activity against both the primary tumor and metastatic spread (Figure 2).
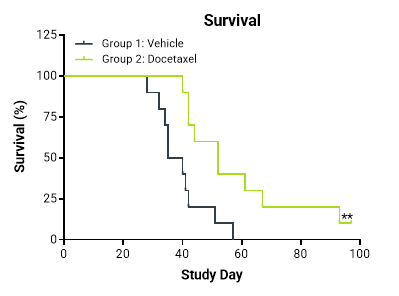
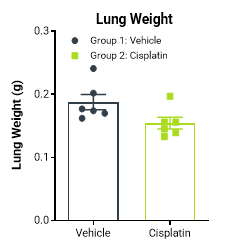
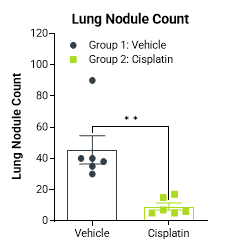
Following surgical resection of the primary tumor, docetaxel treatment produced a statistically significant improvement in survival, while cisplatin significantly reduced lung nodule count at termination (Figure 3).
The ability to quantify lung nodules at endpoint provides a discrete, anatomically grounded readout to complement survival and imaging data.
Together, these findings underscore that the choice between resection and non-resection study designs is itself a meaningful scientific decision, with direct implications for both the clinical scenario being modeled and the type of efficacy data generated.
Figure 2 4T1 Mouse Orthotopic Spontaneous Breast Cancer Metastasis Model Without Resection Of Primary Tumor. Body weight and tumor volume were assessed over 30 days. Tumor volume measured by calipers up to three times per week. Lung weight was recorded on termination. Treatment with Cisplatin significantly reduced the tumor growth (p=0.0024) and terminal lung weights of mice (p=0.0049) compared to vehicle treated mice.
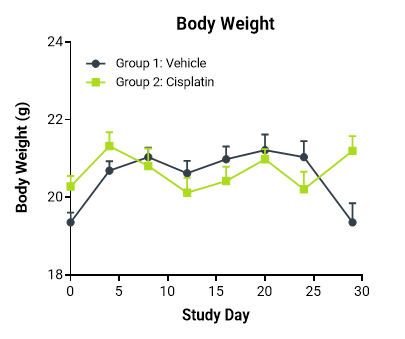
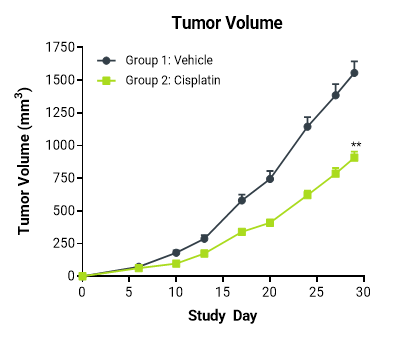
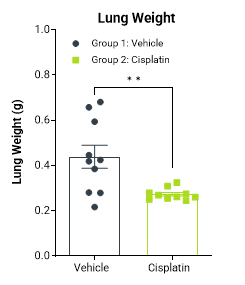
Figure 3 4T1 Mouse Orthotopic Spontaneous Breast Cancer Metastasis Model With Resection Of Primary Tumor. Primary tumors were surgically resected on study day 13. Lung weight and number of lung nodules recorded on termination. A statistically significant reduction in the number of lung nodules in Cisplatin treated mice was observed (p=0.0029)
Experimental Metastasis: Route of Injection as an Organ-Targeting Tool
Where spontaneous metastasis models capture the full metastatic process, experimental metastasis models offer speed and reproducibility by delivering tumor cells directly to the target organ. The injection route is a deliberate experimental variable: different routes direct tumor cells to different organs, allowing studies to be designed around the specific metastatic context of interest.
Intravenous tail vein injection is frequently used to generate lung metastasis models. ChemPartner has validated several syngeneic models using this approach, including the B16-F10-Luc melanoma model established in female C57BL/6 mice, which reproducibly generates pulmonary metastatic lesions (Figure 4). Non-invasive bioluminescence imaging (BLI) enables longitudinal tracking of progressive lesion development from day 1 through to day 22. Lung surface nodule enumeration is available as an additional quantitative endpoint.
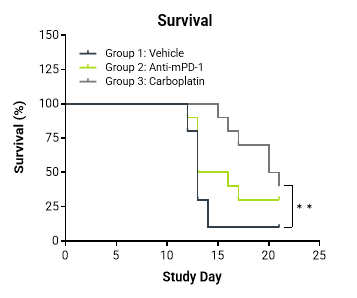
Liver metastasis can be achieved through intrasplenic injection using a hemi-splenectomy design, which preserves residual splenic immune function while directing tumor cells to the liver via the portal circulation. ChemPartner’s CT26-Luc liver metastasis model applies this approach to generate syngeneic hepatic lesions in BALB/c mice (Figure 5).
This model is particularly informative in the context of the site-dependent immunophenotype data described in the previous post (blog link). CT26 tumors are characteristically “hot” in subcutaneous, intracarotid, and intrasplenic settings, yet switch toward a colder phenotype under orthotopic colonic implantation. Extending this characterization to the hepatic metastatic setting enables assessment of whether the immune microenvironment of liver metastases remains permissive to immune checkpoint inhibitor (ICI) activity.
Efficacy data from this model demonstrates a statistically significant reduction in tumor-associated bioluminescence (TABL) following anti-mPD-1 treatment, alongside a significant survival benefit with carboplatin. The ability to track lesion burden longitudinally via BLI, with quantitative imaging across vehicle, anti-mPD-1, and carboplatin cohorts through to day 14, provides a quantitative dataset capturing both the kinetics and magnitude of treatment response.
Across ChemPartner’s systemic metastasis models, injection route, imaging modality, and endpoint selection are tailored to the organ site and underlying biological question, enabling study designs that more closely reflect the specific metastatic context under investigated.
Figure 4 Systemic Metastasis Model With Mouse B16-F10-Luc Melanoma Cell Line. Cell line was sourced from ATCC (parental cell CRL-6475™), Luc-transduced in house. Body weight and total flux were measured to assess tumor progression and location. Progressive increase in bioluminescent signal over the duration of the model.
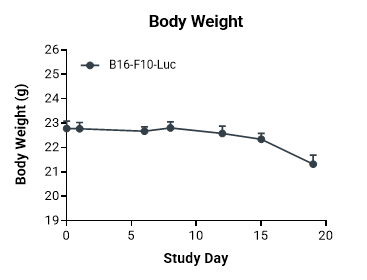
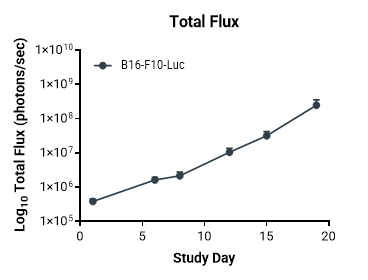
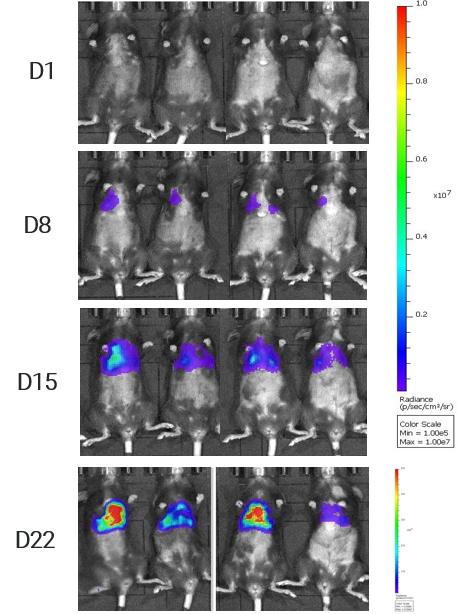
Figure 5 CT26-Luc Mouse Hemi-splenectomy Liver Metastasis Model. Mouse CT26-Luc colon cancer cell line was sourced from ATCC (CRL-2638™, Luc-transduced in – house). Liver metastases modeled following hemi-splenectomy after injection of CT26-Luc cells into the spleen of female BALB/c mice. Median survival time for mice: Vehicle; 13 days, Anti-mPD-1; 14.5 days, Carboplatin; 20.5 days. Carboplatin significantly increases survival in mice compared to vehicle-treated animals (p=0.0027).
Genetically Engineered Mouse Models: Tumor Initiation Through Defined Oncogenic Mutations
Where spontaneous and experimental metastasis models rely on the transplantation of established cell lines, GEMMs take a fundamentally different approach. Tumor formation is driven by defined oncogenic mutations introduced directly into the mouse genome, allowing lesions to arise within their native tissue context from the earliest stages of tumor development. This provides a level of biological fidelity that transplantable models cannot fully replicate, particularly with respect to tumor-stroma interactions, immune editing during tumor evolution, and the progressive remodeling of the tumor immune microenvironment over time.
The KPC model is one of the most clinically relevant preclinical systems for pancreatic ductal adenocarcinoma. It is driven by two of the most common oncogenic alterations in human disease: an activating KrasG12D mutation, which initiates and sustains oncogenic signaling, and a Trp53R172H gain-of-function mutation, which disrupts tumor suppression function and promotes disease progression.
Cell lines derived from KPC GEMM tumors retain many of the defining biological characteristics of the original model while also offering the practical advantages of a transplantable system, including controlled inoculation timing, reproducible growth kinetics, and compatibility with standard efficacy study designs.
CDX Metastatic Models: Extending the Platform to Human Tumor Lines
Where the therapeutic target or antigen of interest is human-specific, cell line-derived xenograft (CDX) models in immunocompromised mice are the appropriate alternative. Rather than serving as competitors to syngeneic systems, CDX metastatic models address a distinct set of experimental questions; collectively the two platforms span a broad range of clinical indications and translational contexts.
ChemPartner’s CDX metastatic portfolio includes models incorporating multiple injection routes and organ-specific metastatic settings. Intraperitoneal implantation of ES-2-Luc human ovarian cancer cell establishes disseminated peritoneal disease in both nude and NOG mice, with bioluminescence imaging confirming multi-organ spread involving liver, intestines, kidneys, and pancreas, alongside development of peritoneal ascites (Figure 6).
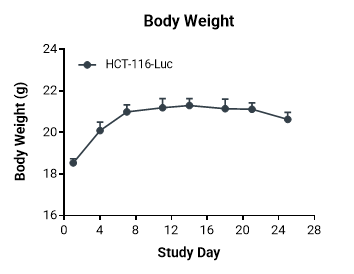
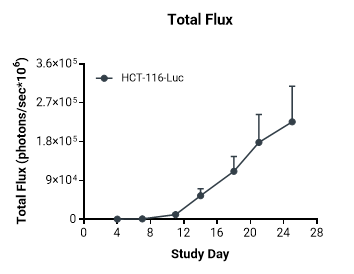
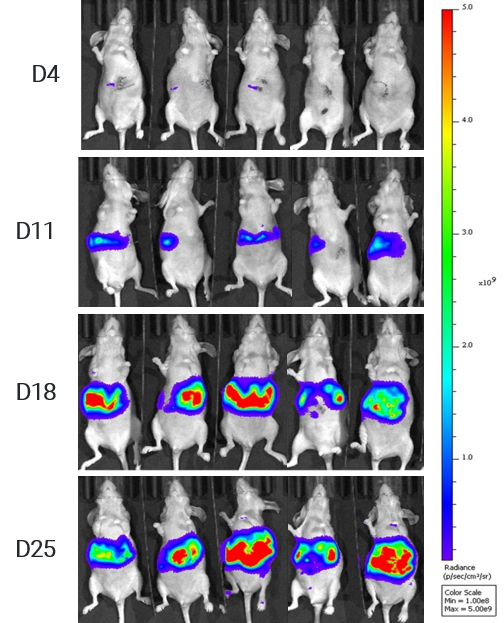
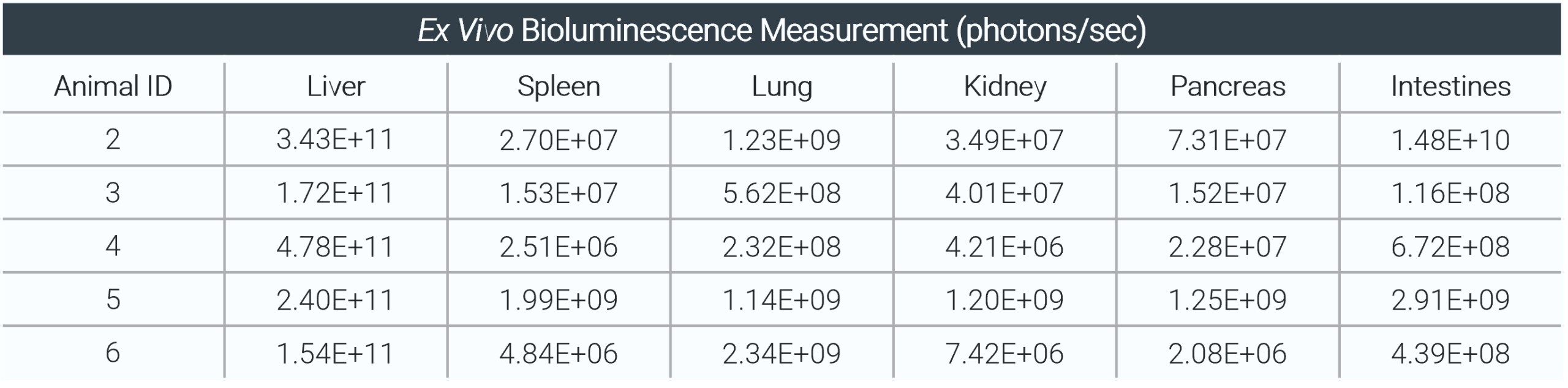
The PC-3-Luc human prostate cancer model generates disseminated bone metastases following intracardiac injection, with evidence of lesions in bone, brain, and lung (Figure 7). In a separate liver metastasis model, hepatic portal vein injection of HCT-116-Luc human colon cancer cells produces targeted liver colonization, with ex vivo BLI confirming organ-level distribution (Figure 8).
Figure 6 ES-2-Luc Human Ovarian Cancer Intraperitoneal Metastasis Model. Human ES-2-Luc ovarian cancer cell line sourced from ATCC and intraperitoneal growth established in female BALB/c nude mice. Body weight maintained for the duration of the study. Evidence of peritoneal ascites attributed to increase in body weight after day 14.
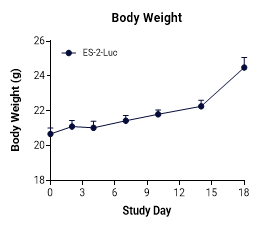
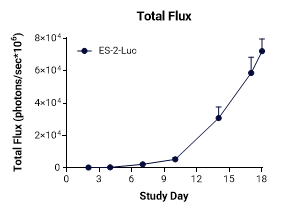
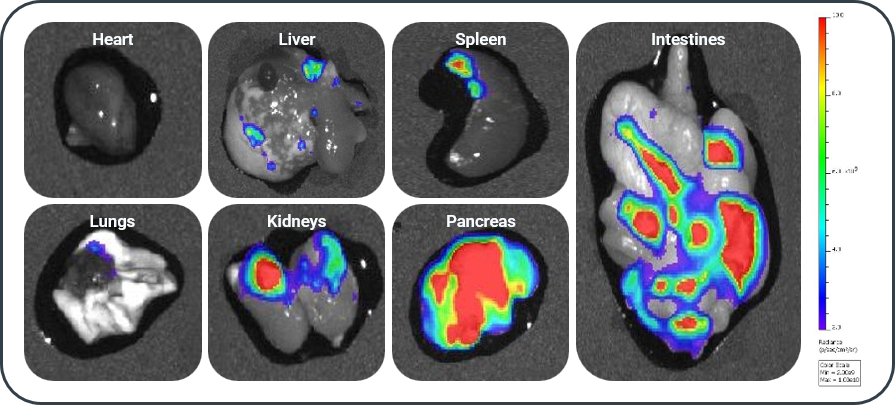
Figure 7 Bone Metastasis Model of Prostate Cancer. Human PC-3-Luc prostate cancer cell line sourced from ATCC and disseminated bone metastases were established following intracardiac injection of PC-3-Luc cells into male BALB/c nude mice. Body weight maintained for the duration of the study. Visible evidence of metastatic lesions in the bone, brain, and lungs.
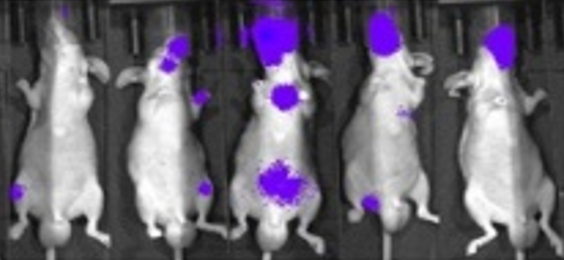
Figure 8 Hepatic Portal Vein Metastasis Model of Colon Cancer. Human HCT-116-Luc colon cancer cell line sourced from ATCC. Metastasis was established following hepatic portal vein injection of HCT-116-Luc cells using female BALB/c nude mice. Body weight maintained for the duration of the study. Evidence of hepatic metastases.
Building the Right Preclinical Strategy
Across this three-part series, each post has addressed a distinct variable in preclinical model selection. Tumor immunophenotype, implantation site, and metastatic context each shape what a model can reveal about ICI biology and therapeutic potential — and each requires deliberate consideration at the study design stage.
A central advantage of syngeneic metastasis models is that these questions can be interrogated in an immunologically intact host, with ICI profiling, immune cell analysis, flow cytometry, IHC, and transcriptomic readouts available to characterize response at the mechanistic level.
ChemPartner’s portfolio spans spontaneous, systemic, and GEMM-derived syngeneic models alongside CDX metastatic models, covering a broad range of indications, organ sites, and experimental settings. To discuss how this platform can support your program, please contact our team.
Let’s Connect!
